


Congenital Spinal Anomalies: Diagnosis and Long-Term Management
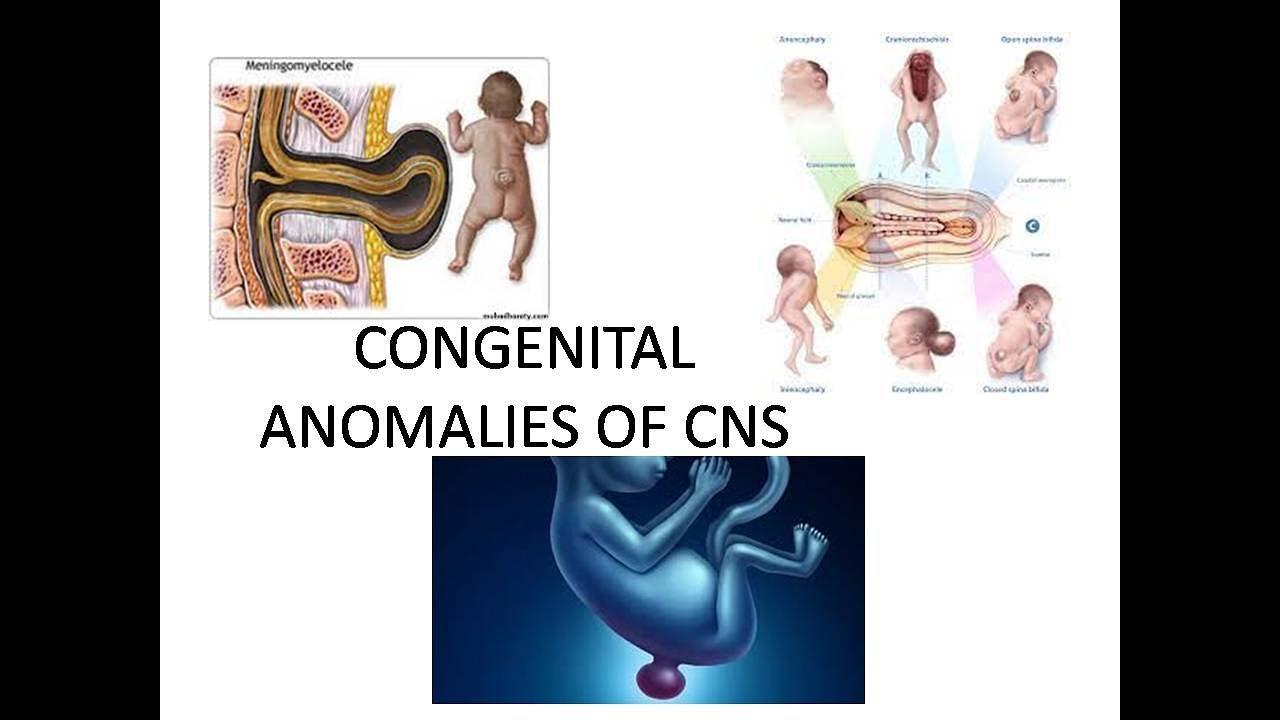
Congenital Spinal Anomalies: Diagnosis and Long-Term Management
Congenital anomalies riyadh represent a diverse range of structural conditions that develop in utero, affecting the formation of the vertebrae and the spinal cord. In Riyadh, the medical landscape has evolved to offer sophisticated prenatal screening and multidisciplinary long-term care, ensuring that children with these conditions can achieve the best possible quality of life. Management is rarely a single event; rather, it is a longitudinal journey that adapts as the child grows from infancy through adolescence.
Understanding the Spectrum of Anomalies
Congenital anomalies of the spine are broadly categorized by whether they affect the bony structure (vertebrae) or the neural tissue (spinal cord).
-
Neural Tube Defects (Spina Bifida): This is perhaps the most well-known category. It ranges from Spina Bifida Occulta (a mild, often invisible gap in the vertebrae) to Myelomeningocele, the most severe form where the spinal cord and nerves are exposed in a sac on the infant's back.
-
Vertebral Formation Defects: Conditions like Congenital Scoliosis occur when the vertebrae do not form as complete rectangles or fail to separate properly, leading to an abnormal sideways curvature.
-
Tethered Cord Syndrome: In this condition, the spinal cord is abnormally attached to the surrounding tissues, preventing it from "floating" freely within the spinal canal. As the child grows, this attachment stretches the cord, potentially causing nerve damage.
-
Diastematomyelia: A rare condition where the spinal cord is split into two longitudinal halves by a bony or fibrous "spur."
The Diagnostic Pathway
In Riyadh’s advanced medical centers, diagnosis often begins before the child is even born, allowing families to prepare for immediate neonatal care.
1. Prenatal Screening
-
Maternal Serum Alpha-Fetoprotein (MSAFP): A blood test conducted around the 16th to 18th week of pregnancy. High levels of AFP can indicate an open neural tube defect.
-
Anatomical Ultrasound: Conducted between 18 and 24 weeks, high-resolution ultrasound can visualize structural defects in the spine and skull.
-
Fetal MRI: In complex cases, a fetal MRI may be used to provide detailed images of the baby’s central nervous system while still in the womb.
2. Postnatal Evaluation
If an anomaly is suspected or diagnosed at birth, the medical team uses a suite of imaging tools to map the defect:
-
X-rays and 3D EOS Imaging: Used primarily to assess the alignment of the vertebrae and the degree of curvature in scoliosis or kyphosis.
-
MRI and CT Scans: These are essential for looking at the spinal cord, identifying tethered cords, and checking for associated brain anomalies like Hydrocephalus (fluid accumulation).
-
Renal and Cardiac Ultrasound: Because spinal anomalies often occur alongside kidney or heart issues, these screenings are standard practice in a comprehensive evaluation.
Long-Term Management Strategies
Management is a marathon, not a sprint. The goal is to maximize function, prevent neurological decline, and manage secondary complications.
1. Surgical Intervention
-
Neonatal Closure: For infants with Myelomeningocele, surgery is typically performed within 24 to 48 hours of birth to close the defect and protect the exposed nerves from infection and trauma.
-
Release of Tethered Cord: If a child shows signs of nerve stretching (such as leg weakness or bladder changes), surgeons perform a procedure to detach the cord from the spinal canal.
-
Growing Rods and Fusion: For progressive congenital scoliosis, "growing rods" can be used to control the curve while allowing the spine to continue growing. Once skeletal maturity is reached, a permanent spinal fusion may be performed.
2. Multidisciplinary Care
Leading centers in Riyadh utilize a team-based approach, which is critical for long-term success:
-
Urology: Managing "neurogenic bladder" is a lifelong priority. This includes regular ultrasounds and, if necessary, clean intermittent catheterization to protect kidney health.
-
Orthopedics: Monitoring for hip dysplasia, foot deformities (like clubfoot), and scoliosis as the child grows.
-
Physical and Occupational Therapy: Focused on maintaining muscle strength, improving balance, and training the child to use assistive devices like braces or wheelchairs.
-
Neurosurgery: Monitoring for signs of shunt malfunction if the child has hydrocephalus.
The Role of Folic Acid in Prevention
While many causes of spinal anomalies remain unknown, the link between Folic Acid deficiency and neural tube defects is well-established. Health authorities in Saudi Arabia strongly recommend that women of childbearing age take 400 micrograms of folic acid daily before and during early pregnancy. For women with a history of a previous child with a spinal defect, higher doses may be prescribed under medical supervision.
Moving Toward Adulthood: Transitional Care
As a child with a congenital spinal anomaly approaches adulthood, the focus shifts toward "Transitional Care." This process involves moving the patient from pediatric specialists to adult-focused physicians who can manage long-term neurological and urological health. The objective is to ensure the individual remains independent, mobile, and healthy throughout their adult life.
Through the combination of early surgical repair, vigilant monitoring, and integrated therapies, the outlook for children born with spinal challenges has never been more promising. The journey is supported by a community of experts dedicated to ensuring that every child can stand, move, and thrive.
Categorie
Leggi tutto
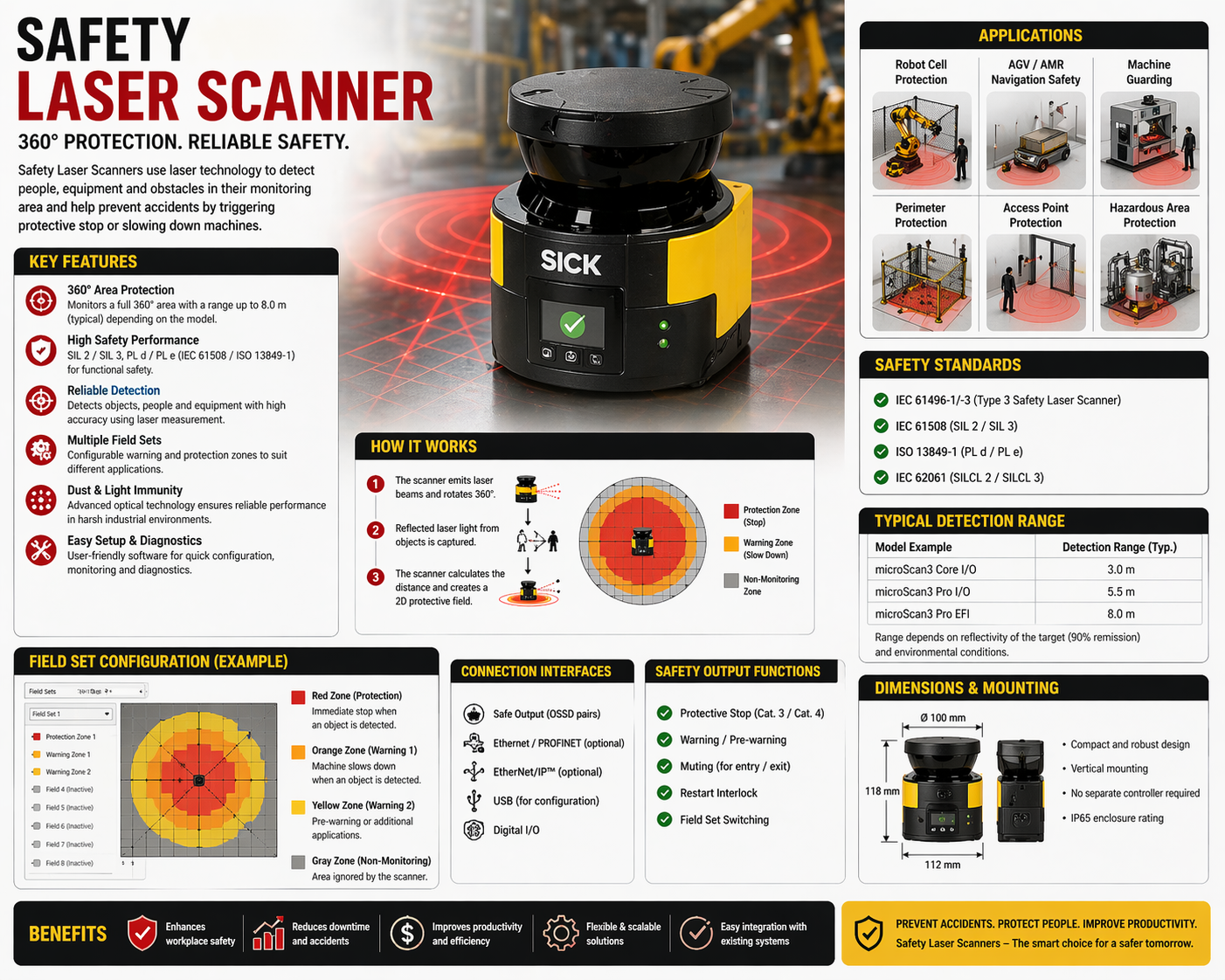
With the global focus on enhancing workplace safety, the demand for industrial safety laser scanners has surged dramatically. Market research indicates that the Safety Laser Scanner Market Size is projected to reach approximately $2.76 billion by 2035, reflecting a robust compound annual growth rate (CAGR) of 10.24%. This growth trajectory underscores the increasing adoption of laser...
Damascus steel knives have a kind of magic about them. People are drawn to their beauty, but they stick around for how well these knives actually work. The wavy, mesmerizing patterns catch the eye, but it’s the razor-sharp edge and lasting toughness that make them a kitchen favorite. These knives come with centuries of history and still manage to feel modern, blending function and...
전용 파워볼사이트를 찾고 있다면 단순한 추천이나 광고성 정보가 아닌, 실제로 도움이 되는 기준과 판단 방법이 필요합니다. 이 글에서는 파워볼사이트 추천 를 선택할 때 무엇을 기준으로 삼아야 하는지, 어떤 요소가 중요한지, 그리고 왜 이러한 선택이 장기적인 결과에 영향을 미치는지를 구체적으로 설명합니다. 독자는 이 글을 통해 보다 안전하고 안정적인 환경을 선택하는 데 필요한 명확한 기준을 얻을 수 있습니다. 전용 파워볼사이트란 무엇인가 전용 파워볼사이트는 특정 사용자 경험을 중심으로 설계된 플랫폼을 의미합니다. 일반적인 사이트와 달리 이용자의 편의성과 안정성을 고려한 구조를 갖추고 있으며, 보다 집중된 서비스 환경을 제공합니다. 이러한 사이트는...
The mobile virtual network operator market dynamics are witnessing a significant transformation as service providers adapt to the ever-evolving telecommunications landscape. Currently valued at approximately $58.1 billion, the market is projected to expand to $89.96 billion by 2035, reflecting a compound annual growth rate (CAGR) of 3.71%. This growth is driven by the increasing...

When it comes to fostering deeper intimacy and overcoming challenges in romantic relationships, consulting a Sexologist in Riyadh, Jeddah & Saudi Arabia can be transformative. Many couples struggle with communication gaps, emotional distance, or diminished desire, and these issues often impact overall well-being. Expert sexual therapy focuses not only on physical aspects of intimacy but...

